Management of Bariatric Complications: An American Gastroenterological Association Clinical Practice Update
Vanessa M. Shami, MD, FASGE, reviewing Kumbhari V, et al. Clin Gastroenterol Hepatol 2021 Mar 16.
More than 200,000 bariatric surgeries took place in 2018. Of these, 95% were either a sleeve gastrectomy or Roux-En-Y gastric bypass. Although the 90-day mortality rate from bariatric/metabolic surgery is very low (0.1%-0.3%), the overall complication rate is 7% to 10% (4% being major complications). Treatment algorithms for complications have not been standardized due to a lack of prospective studies for deciding the best approach for these patients. This practice update from the American Gastroenterological Association attempts to bridge this knowledge gap through expert review and a focus on complications within the first 90 days after bariatric intervention.
Below are notable points from all 7 best practice recommendations:
- Endoscopic approaches should be done in a multidisciplinary manner, with bariatric surgery and interventional radiology (IR) comanaging the patient with daily communication.
- Endoscopists should have comprehensive knowledge of the indications, contraindications, risks, benefits, and outcomes of various endoscopic treatment techniques as well as the risks and benefits of surgical and IR approaches.
- Clinicians should feel comfortable with interventional endoscopy techniques, including concomitant fluoroscopy, stent deployment and retrieval, stenosis management, and percutaneous drain management.
- Patients should undergo comorbid medical (nutrient deficiencies, infections, pulmonary embolism) and psychological (depression, anxiety) screening before endoscopic intervention.
- Endoscopic approaches to managing bariatric/metabolic surgery complications may be considered for patients in the immediate, early, and late postoperative periods, depending on hemodynamic stability.
- Clinicians should have a detailed understanding of the pathophysiologic mechanisms initiating and perpetuating conditions, such as staple-line leaks, to allow for a prompt diagnosis and appropriate therapy targeted not only at the area of interest but also any concomitant downstream stenosis.
- Clinicians should recognize that the goal for endoscopic management of staple-line leaks is often not necessarily the initial closure of the leak site but, instead, to promote drainage of material from the perigastric collection into the gastric lumen so that the leak site closes by secondary intention.

COMMENTThese authors have highlighted the importance of using a multidisciplinary approach, appreciating the pathophysiologic mechanisms of leaks, and having a solid foundation of interventional endoscopy techniques before embarking on the endoscopic management of bariatric complications. This review also offers a treatment algorithm (Figure 1) and emphasizes how our endoscopic approach depends on the size of the leak (<10 mm vs >10 mm), timing from surgery (<6 weeks vs >6 weeks), and any downstream stenosis. Hopefully, future studies can build on this algorithm as endoscopic techniques advance for these patients.
Note to readers: At the time we reviewed this paper, its publisher noted that it was not in final form and that subsequent changes might be made.
CITATION(S)
Kumbhari V, Cummings DE, Kalloo AN, Schauer PR. AGA clinical practice update on evaluation and management of early complications after bariatric/metabolic surgery: expert review. Clin Gastroenterol Hepatol 2021 Mar 16. (Epub ahead of print) (https://doi.org/10.1016/j.cgh.2021.03.020)
Ähnliche Beiträge
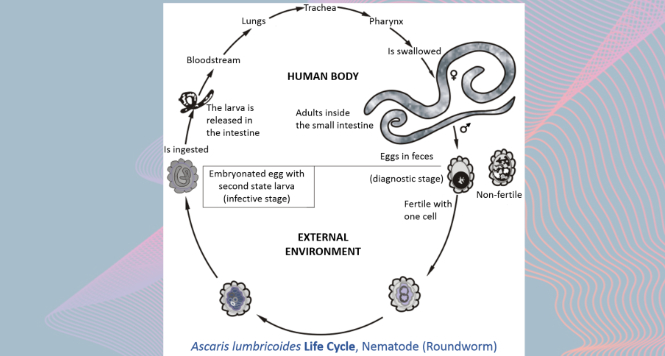
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations
VIEW THE GALLERY
Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal
