Diagnosis and Management of Atrophic Gastritis: Clinical Practice Update From the American Gastroenterological Association
Vanessa M. Shami, MD, FASGE, reviewing Shah SC, et al. Gastroenterology 2021 Aug 25.
Patients with atrophic gastritis (AG) are at increased risk for gastric cancer; however, the diagnosis and surveillance of AG are not well-defined. Algorithms for the diagnosis and management of AG have not been standardized due to a lack of prospective studies to determine the best approach for these patients. This practice update from the American Gastroenterological Association attempts to bridge this knowledge gap through evidence from published data and expert review.
Best Practice Advice:
- AG is a histologic diagnosis confirming the loss of gastric glands secondary to Helicobacter pylori infection or autoimmune process.
- The presence of intestinal metaplasia (IM) implies the diagnosis of AG.
- Typical features of AG include pale gastric mucosa, increased visibility of vasculature secondary to thinning mucosa, and loss of gastric folds. IM appears as light blue crests and white, opaque fields.
- Biopsy specimens should be taken, at a minimum, from the antrum/incisura and body to determine the extent of AG.
- When autoimmune gastritis (AIG) is diagnosed, antiparietal cell antibodies and anti-intrinsic factor antibodies, in addition to vitamin B12 and iron levels, should be checked.
- Patients with AG should be assessed and, if positive, treated for H Pylori, followed by confirmation of eradication.
- Surveillance every 3 years with EGD should be considered in patients with advanced AG (based on histologic grade and extent).
- The surveillance interval for AIG should be based on individualized assessment and shared decision- making.
- Pernicious anemia is a late manifestation of AIG. In newly diagnosed patients, endoscopic regional biopsies should be performed to confirm corpus-predominant AG for risk stratification and to rule out prevalent gastric neoplasia, including neuroendocrine tumors (NETS).
- Patients with AIG should be screened for type 1 NETs, and NETS <1 cm should be resected. Endoscopic surveillance should be performed every 1 to 2 years.
- Vitamin B12 and iron levels should be checked in patients with AIG. Likewise, the diagnosis of AIG should be entertained in patients with vitamin B12 and/or iron deficiency.
- Patients with AIG should be screened for thyroid disease.

COMMENTThese authors have highlighted the importance of the recognition, diagnosis, and management of AG.
Note to readers: At the time we reviewed this paper, its publisher noted that it was not in final form and that subsequent changes might be made.
CITATION(S)
Shah SC, Piazuelo MB, Kuipers EJ, Li D. AGA clinical practice update on the diagnosis and management of atrophic gastritis: expert review. Gastroenterology 2021 Aug 25. (Epub ahead of print) (https://doi.org/10.1053/j.gastro.2021.06.078)
Ähnliche Beiträge
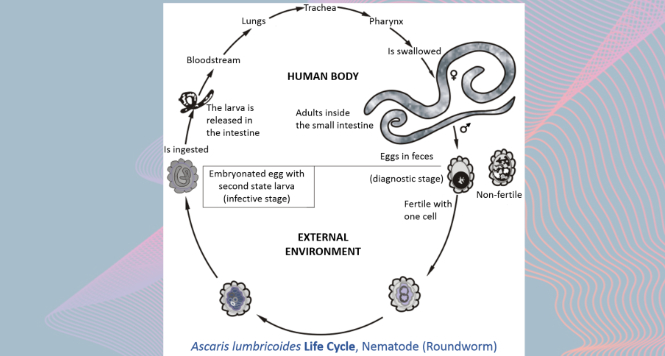
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations
VIEW THE GALLERY
Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal
