Key to Optimal Pathology Reporting for Endoscopic Gastric Cancer Resection Specimens
Vanessa M. Shami, MD, FASGE, reviewing Shi C, et al. Gastroenterology 2021 Nov 11.
Endoscopic resection (ER) of early gastric neoplasia is being performed with increasing frequency by endoscopists. Complete and accurate reporting of pathology is imperative to provide optimal follow-up care. This involves thorough reporting on the part of both the endoscopist as well as the pathologist. The International Collaboration on Cancer Reporting recently published an evidence-based international pathology reporting dataset for ER of early gastric cancers. The elements are categorized as core (required) or noncore (recommended).
Core elements to include in pathology reporting:
- Communication of clinically relevant information, including the endoscopic procedure performed (endoscopic mucosal resection vs endoscopic submucosal dissection vs etc) and tumor site.
- Specimen description, including tumor dimensions, presence of different tissue layers, as well as tumor focality.
- Tumor type, based on the World Health Organization classification, and tumor grade, according to the Union for International Cancer Control (UICC)/American Joint Committee on Cancer (AJCC) staging systems.
- Depth of invasion, if applicable, and tumor stage, determined using the UICC/AJCC staging systems.
- Lymphovascular invasion for invasive cancers.
- Margin status.
- Neuroendocrine marker expression and Ki-67 proliferation index for carcinomas with neuroendocrine differentiation.
Noncore elements recommended to include in pathology reporting:
- Additional relevant clinical information.
- Macroscopic tumor type (ie, superficial, excavated, etc).
- Coexistent pathology (ie, presence of Helicobacter pylori, atrophic gastritis, etc).
- Epstein-Barr virus, particularly for proximal cancers, and microsatellite instability status when Lynch syndrome-associated gastric cancer is suspected.

COMMENTThe management of patients who have undergone ER for gastric cancers is determined based on pathologic staging, making adequate reporting of specimens imperative. The responsibility in reporting lies with both the endoscopist and pathologist. For the endoscopist, providing details about the resection method and lesion location is required, and reporting relevant clinical information and macroscopic tumor type is recommended. As endoscopists, we should do our part to facilitate good reporting to make the best-informed management decision for our patients.
Note to readers: At the time we reviewed this paper, its publisher noted that it was not in final form and that subsequent changes might be made.
CITATION(S)
Shi C, Webster F, Nagtegaal ID, on behalf of the Dataset Authoring Committee for the development of the ICCR Dataset for Pathology Reporting of Gastric Endoscopic Resections. Pathology reporting of gastric endoscopic resections: recommendations from the International Collaboration on Cancer Reporting. Gastroenterology 2021 Nov 11. (Epub ahead of print) (https://doi.org/10.1053/j.gastro.2021.11.010)
Ähnliche Beiträge
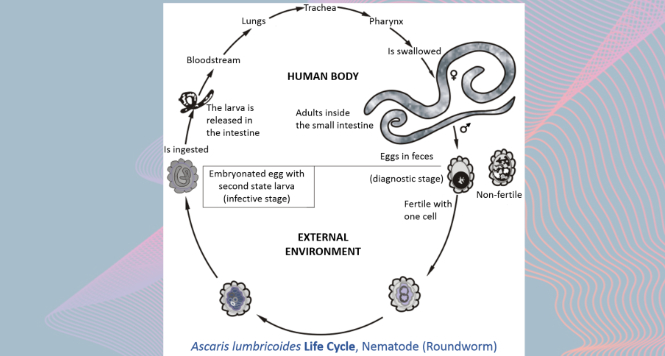
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations
VIEW THE GALLERY
Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal
