Barrett’s carcinoma at the Z-line
Prof. Dr. Mario Anders
Vivantes Wenckebach Klinikum, Berlin
Patient history
Presentation, for a second opinion, of a 47-year-old male patient with multiple morbidities, in whom an early Barrett’s carcinoma had previously been removed using endoscopic mucosal resection (EMR) at an external hospital (pT1b, pL0, pL0, pV0, pR1 also at base). Despite the R1 situation at the base and the patient’s age, a surgical intervention had not been carried out due to the patient’s poor general condition and concomitant conditions.


Endoscopic images
There was an initially noticeable bulge at the Z-line; on closer examination, an irregular central area was then seen, with a suspicion of undermining growth under the squamous epithelium.

Endoscopic therapy
The planned endoscopic resection starts with marking of the lesion with a sufficient safety margin.


Status post endoscopic submucosal dissection (ESD), including all markings.

Histology
Submucosal invasion by a T1b carcinoma (sm1, max. 160 µm), L0, V0, R0, G1, with growth partly undermining the squamous epithelium.
Further procedure
Presentation of the case at the interdisciplinary tumor board. Surgery was not planned, due to the patient’s multiple morbidities. Follow-up (with endoscopy and CT).

Related Posts
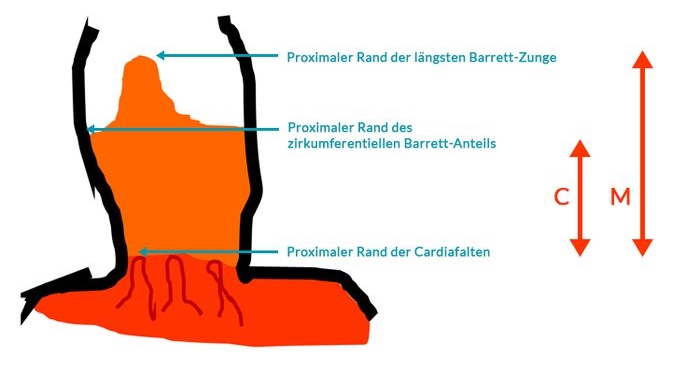
Prague classification
The Prague classification was presented by an international research group
VIEW THE CLASSIFICATION